

Clinical Tips, Diagnosis of Pulpal Pathology
Back when I was working as an Endodontist with the Australian Navy, I often mentored newly graduated dentists. There was an interesting interaction between us that would often occur. The junior dentist would come into my surgery with a question about diagnosis. They would explain a set of symptoms and then show me a radiograph. I would then ask what the pulp test result was. The new grad would then slowly back out of the room in order to return to the patient and conduct the test.
I’m not sure why the pulp testing was left off the list, but I hope I hope that by the time the junior dentist had finished their posting and moved on to a new posting that pulp testing is one of the most important tools allowing us to to diagnose. Unfortunately, there is nothing certain when it comes to pulpal diagnosis, especially when we get to the grey area of reversible/irreversible pulpitis. If we really want to know what’s happening in the pulp and periapical area of a tooth, we need to extract it, section it, and look at it under a microscope. But that’s not practical…….
Pulp testing is not 100% accurate. If it was, then diagnosis would be much easier, but it often gives us essential information that will confirm a clinical diagnosis. When it comes to vital pulps, electric and cold testing gives a positive result 81-86% of the time (Petersson & Kiani-Anaraki, 1999). In a partially or completely necrotic tooth, these modalities will give a negative result on almost all occasions. This is useful infromation to have at hand.
Here is an example from when I was doing my post-graduate training:
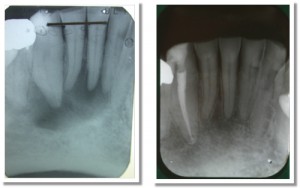
Compare these radiographs. The image on the left is the pre-op and the image on the right is the two year review.
In the case above, we can see there is a definite lucency surrounding the lower right canine and central incisor. The lateral incisor may also be involved. Pulp testing with both cold and EPT revealed the canine was testing negative and the incisors were testing positive. As only the canine was testing negative, I only treated the canine. At the two year review, we can see that the lesion has healed and normal periradicular architecture has been re-formed around the vital incisors. If we just worked from the x-rays, we’d probably treat all three teeth, and subject the patient to unnecessary treatment. This is a pretty simple lesson.
Here are the keys to successful pulp testing:
1. Make sure the teeth are completely dry and isolated with cotton wool rolls;
2. Place the tip of the pulp tester on tooth structure, not restoration, and use a small (perhaps half of a) cotton pellet or endo sponge;
3. Start your test with a tooth that you expect will give a normal result and is not involved with the area in question. This will allow the patient to get a feel for what a normal response is;
4. Test with both cold and EPT. If the patient is experiencing symptoms such as a hyper-response to hot foods/liquids, then use hot as well.
In my surgery I have the pulp tester sitting right next to me, along with things like the apex locator and endo motor. We use it that often.
Petersson KS, C. Kiani-Anaraki, M. Evaluation of the ability of thermal and electrical tests to register pulp vitality Endod Dent Traumatol 1999;15:127-131.
Hi Pat, First of all, excellent, excellent endo blog! One of the bad habits that I picked up once I had left dental school was to make a diagnosis based primarily on radiographic signs and the patient’s reported symptoms. Soon enough, though, I ran into several puzzling cases. Pulp testing is vitally important! (No pun intended :P)
Dentist in the northThx for the interesting read.
Always trying to improve my diagnostic capabilities, and this was an article that will help for sure.
Any suggestions on what type of EPT unit to use.
Hi Guys, Thanks for the comments. I happen to use the Sybron Endo Analytics electric pulp tester. Mainly because it combines apex locator and pulp tester into one unit, reducing the number of machines we need to have. Also, it comes with some nice tips for getting under crown margins. Pat